Oral Contraceptives’ Effect on Menstruation-Related Aggression in Children with Autism Spectrum Disorder
AUTHORS:
David Matsibekker, MD1; Ruchita Kachru, MD2; Bilal Khodr, MD1; Mary Valletta, MD1; Sebastian Cuitiva, PA3; Sanjeev Tuli, MD4
1Assistant Professor, Department of Pediatrics, University of Florida, Gainesville, Florida
2Associate Professor, Department of Pediatrics, University of Florida, Gainesville, Florida
3Physician Assistant, Department of Pediatrics, University of Florida, Gainesville, Florida
4Professor and Chair, Department of Pediatrics, University of Texas Medical Branch, Galveston, Texas
REVIEW ARTICLE | PUBLISHED Spring 2026 | Volume 46, Issue 2
DOWNLOAD PDF
Abstract
Individuals with autism spectrum disorder often experience heightened difficulty managing menstrual symptoms, including increased aggression and self-injurious behaviors. Sensory sensitivities and limited communication abilities can exacerbate these behaviors. This case report evaluates the impact of oral contraceptive therapy on aggression associated with menstruation in post-menarche females with autism spectrum disorder. Three female patients with autism spectrum disorder and documented menstruation-related aggression were followed over an 8–10-month period after initiation of hormonal contraceptive therapy. The Modified Overt Aggression Scale was used to assess behavioral changes. All three patients demonstrated a significant reduction in aggression scores following hormonal therapy, with decreases ranging from 16 to 22 points. Menstrual suppression was achieved in all patients without adverse effects. Hormonal contraception may represent a viable adjunct therapy for managing menstruation-related aggression in females with autism spectrum disorder. Larger, prospective studies are warranted to validate these findings.
Introduction
Menstruation can present significant behavioral and emotional challenges for individuals with autism spectrum disorder (ASD). These challenges, including severe premenstrual syndrome (PMS) and dysmenorrhea, are often magnified by sensory sensitivities, communication deficits, and behavioral dysregulation. Notably, menstruation may exacerbate aggressive and self-injurious behavior, particularly in non-verbal or minimally verbal patients.1-2
Premenstrual dysphoric disorder (PMDD) is a severe, mood-related condition that is more commonly reported among individuals with ASD than in the general population, with reported prevalence ranging from 14% to 92% in some cohorts. Symptoms include irritability, mood swings, aggression, and social withdrawal.4-6
The American College of Obstetricians and Gynecologists (ACOG) supports menstrual suppression in individuals with cognitive or physical disabilities who desire or require fewer menses.⁷ However, there is limited literature that has explored the impact of hormonal therapy on menstruation-related aggression in females with ASD.
This case report describes the clinical course of three adolescent females with ASD and aggression exacerbated by menses who were treated with oral contraceptive therapy and monitored using the Modified Overt Aggression Scale (MOAS).8
Case Presentations
Case 1: An 11-year-old female with ASD (Level 3 support needs) and intellectual disability presented with severe behavioral disturbances coinciding with menstruation. Her aggression, including hitting, head banging, and property destruction, recurred with each menstrual cycle. Baseline R-MOAS score was 30. Despite behavioral therapy and pharmacologic treatment (aripiprazole, clonidine, stimulants), symptoms persisted. Following insurance-related delays, she was initiated on a continuous progestin-only pill (norethindrone 0.35 mg). Within one month, physical aggression ceased, though emotional dysregulation persisted intermittently. By 10 months, menstrual suppression was achieved, and R-MOAS had decreased to 8.
Case 2: A 12-year-old female with ASD and a history of aggression during menstruation was noted to become verbally threatening and physically aggressive during the week preceding menses. Baseline R-MOAS was 23. She had previously been stable on dexmethylphenidate, guanfacine, and hydroxyzine. Hormonal therapy was initiated with norethindrone-ethinyl estradiol (0.4 mg/35 mcg) with quarterly withdrawal bleeding. After 10 months, she showed significant improvement, with verbal threats persisting, but no physical aggression or property destruction. R-MOAS was reduced to 7.
Case 3: A 12-year-old female with ASD and behavioral exacerbations during menstruation exhibited aggression, including punching walls, dangerous outbursts, and auto-aggression. The initial R-MOAS score was 26.
She was first trialed on depot medroxyprogesterone (Depo-Provera®), but it was discontinued due to side effects and lack of amenorrhea. She was then transitioned to a combined oral contraceptive (levonorgestrel-ethinyl estradiol with quarterly placebo dosing). After 10 months, aggression reduced significantly, with only verbal threats and gestures noted. Her R-MOAS score dropped to 7.
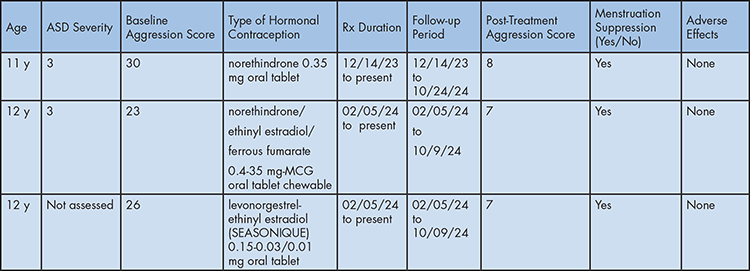
Summary of Oral Contraception Effect on Menstruation-Related Aggression in the Context of ASD
Discussion
This case report provides preliminary evidence that hormonal contraception may reduce menstruation-related aggression in adolescent females with ASD. MOAS scores of three patients with ASD decreased after the initiation of hormonal therapy, correlating with behavioral improvement and successful menstrual suppression.
Aggression in ASD is a major cause of caregiver burden and increases the risk of psychiatric hospitalization and injury. Existing literature indicates that females with ASD are more prone to PMDD and related behavioral challenges.1,5,6,9–11 However, the role of hormonal modulation in behavioral symptomatology remains underexplored.
Our findings align with ACOG recommendations supporting menstrual suppression in individuals with disabilities and highlight the need for clinicians to consider hormonal interventions as part of the broader treatment strategy in this population.⁷
Limitations of this report include small sample size, lack of control group design, and reliance on parent-reported outcomes. Variability in hormonal agents used also limits direct comparison across these patients. Nonetheless, the consistent reduction in aggression and absence of adverse effects strengthen the rationale for further investigation.
Conclusion
This case report demonstrates that hormonal contraception may reduce perimenstrual aggression in post-menarche adolescents with autism spectrum disorder. Our three patients showed substantial reductions in aggression scores and improved quality of life, with no adverse events reported. These results support the consideration of hormonal therapy as an adjunctive treatment in managing menstruation-related behavioral dysregulation in females with ASD. Larger, controlled studies are needed to validate these findings and inform standardized treatment protocols.
Author(s) Disclosure Statement: The authors report no disclaimers or conflicts of interest.
References
- Steward R, Crane L, Roy EM, Remington A, Pellicano E. “Life is much more difficult to manage during periods”: Autistic experiences of menstruation. J Autism Dev Disord. 2018;48(12):4287-4292.
- Groenman AP, Torenvliet C, Radhoe TA, et al. Menstruation and menopause in autistic adults: Periods of importance? Autism. 2022;26(6):1563-1572.
- Ames JL, Anderson MC, Cronbach E, et al. Reproductive healthcare in adolescents with autism and other developmental disabilities. Am J Obstet Gynecol.
- Hamilton A, Marshall MP, Murray PJ. Autism Spectrum Disorders and Menstruation. J Adolesc Health. 2011;49(4):443-445.
- Obaydi H, Puri BK. Prevalence of premenstrual syndrome in autism: A prospective observer-rated study. J Int Med Res. 2008;36(2):268-272.
- Lee DO. Menstrually related self-injurious behavior in adolescents with autism. J Am Acad Child Adolesc Psychiatry. 2004;43(10):1193.
- ACOG Clinical Consensus No. 3. General approaches to medical management of menstrual suppression. Obstet Gynecol. 2022;140(3):528.
- Suris A, Lind L, Emmett G, et al. Measures of aggressive behavior: overview of clinical and research instruments. Aggress Violent Behav. 2004;9(2):165-227.
- Burke LM, Kalpakjian CZ, Smith YR, Quint EH. Gynecologic issues of adolescents with Down syndrome, autism, and cerebral palsy. J Pediatr Adolesc Gynecol. 2010;23(1):11-15.
- Cummins C, Pellicano E, Crane L. Supporting minimally verbal autistic girls with intellectual disabilities through puberty. J Autism Dev Disord. 2020;50(7):2439-2448.
- Lever A, Geurts HM. Psychiatric co-occurring symptoms and disorders in adults with ASD. J Autism Dev Disord. 2016;46Bottom of Form