Not All Posterior Rib Fractures are Non-Accidental Trauma: Birth Records, Timing of Injury, and Time to Diagnosis Remain Paramount
AUTHORS:
Cameron M. Rosenthal, MD; Madelin Schneck, MD; Dillon Joiner, MD
Department of Pediatrics, University of Florida, Gainesville
RESIDENT ARTICLE | PUBLISHED SPRING 2022 | Volume 42, Issue 2
DOWNLOAD PDF
CASE REPORT
Patient 1: A 5-day-old male was transferred from an outside hospital due to concern for non-accidental trauma after three rib fractures were found on X-ray.
History of Presenting Illness
The infant was born via induced vaginal delivery at full term with mother reporting a very difficult delivery. After delivery, a bruise on his left arm and bruising of his abdomen were seen on physical examination. On day of life 1, the infant was increasingly fussy and inconsolable, and the maternal grandmother heard a “popping noise on his left side.”. On day of life 2, new-onset crepitus was noted over the chest wall, at which point x-rays were ordered which showed a non-displaced fracture of the 6th rib on the left side and a mildly displaced fracture of the 7th and 8th rib on the left side (Figure 1). The infant was then transferred for further management and evaluation by our institution’s child abuse team.
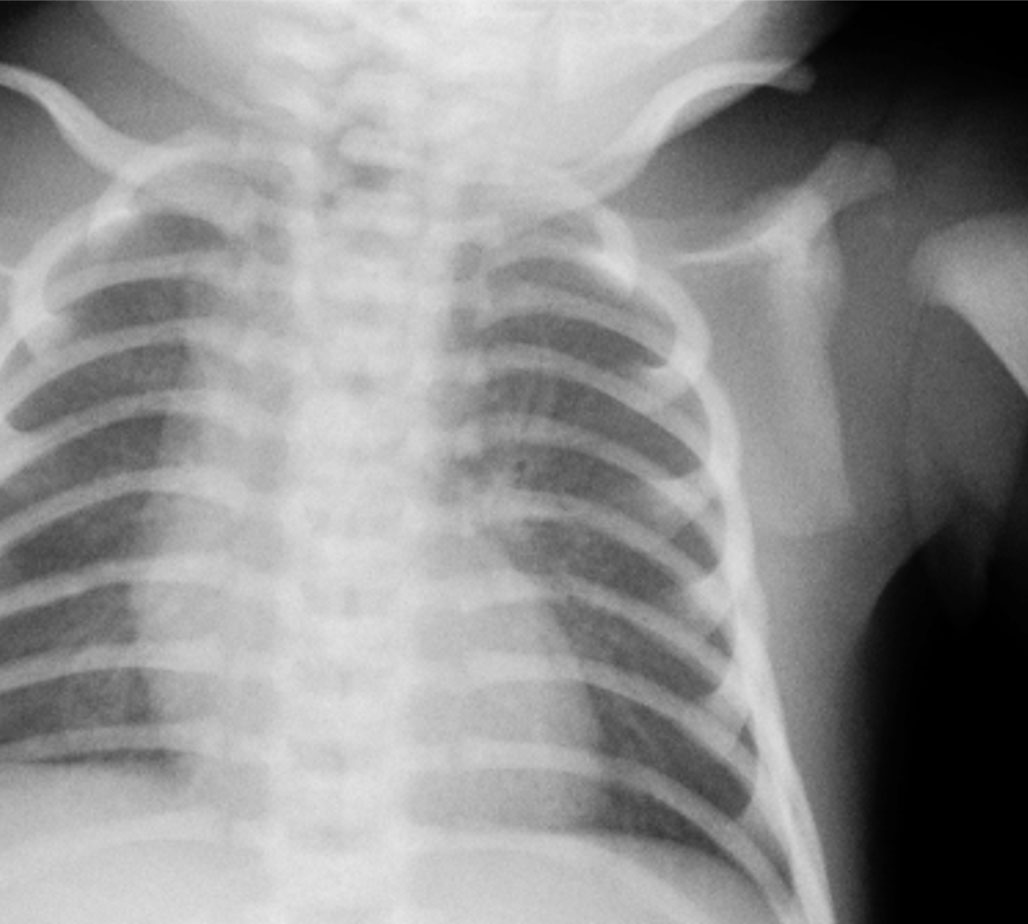
Figure 1
Physical Exam
Birth exam was remarkable only for “bruising to full left forearm.” Upon hospital transfer, the patient was alert and interactive with no acute distress. His length was 52 cm (85th percentile for age and sex) and weight was 3.912 kg (85th percentile). The only remarkable finding was faint purple bruising along the left forearm (Figure 2).

Figure 2
Consultations/Additional Studies
The obstetrician present at delivery was consulted and indicated no traumatic events occured during delivery that could have caused the rib fractures. However, upon review of medical records, the delivery was noted as “a significantly difficult birth and had evidence of some birth trauma with a bruise on the left forearm…per nursing staff, baby was ‘stuck’ for a little while.”
After hospital transfer, a skeletal survey was performed which showed no additional fractures. Head MRI and ophthalmologic evaluation was completed and “suspect optic disc splinter hemorrhage in right eye secondary to birth trauma” was documented in the record.
Diagnosis: Multiple rib fractures due to birth trauma
Patient 2: A 16-week-old male was admitted to the hospital for concern of non-accidental trauma after 8 rib fractures were noted on chest x-ray obtained at routine cardiology follow-up in clinic.
History
The infant was born prematurely at 32 weeks’ gestation via spontaneous vaginal delivery. His mother was unaware that she was pregnant and received no prenatal care. He was transferred to the NICU at a tertiary center due to respiratory distress at birth requiring intubation. He was also noted at birth to have, as noted in the medical record, “significant bruising to chest, abdomen, and face” at delivery. He was discharged home in the care of his mother after a 10-week NICU admission. During the course of this hospitalization, he was found to have a ventricular septal defect, poor feeding, and a small brain hemorrhage on head ultrasound, assumed to be associated with prematurity. He was seen in the cardiology clinic for follow-up one month after discharge, where a chest x-ray was obtained that showed multiple bilateral rib fractures in various stages of healing. He was then admitted to our institution.
Physical Exam
Exam at our institution showed an infant measuring 19.6 inches (< 3rd percentile, adjusted for prematurity), weighing 7 lb 5.5 oz (< 5th percentile, adjusted for prematurity), with head circumference 13.9 in (< 3rd percentile, adjusted for prematurity). Auscultation of the chest revealed a loud systolic murmur. Musculoskeletal/skin exam showed no bruising, crepitus, bony deformity, or other outward signs of trauma.
Consultations/Additional Studies
NICU records from the referring hospital, including multiple chest x-rays, were provided at our request and reviewed by our pediatric radiologists. None of these records showed evidence of fracture after re-review by the child abuse team.
Skeletal survey, head CT, and eye exam were performed upon admission. Skeletal survey revealed left lateral rib fractures involving the 6th, 7th, 8th, 9th, and 10th ribs with abundant callus, as well as more acute fractures of the right lateral 7th, 8th, and 9th ribs that did not show signs of healing. No additional fractures were seen. Head CT and ophthalmologic exam revealed no further signs of trauma.
Diagnosis: Physical abuse
Discussion
Most rib fractures in infants are the result of child abuse or non-accidental trauma.1,2 These fractures result from the anterior-posterior compression by an adult squeezing the infant’s chest with the greatest force occurring over the transverse process. However, as these two cases contrast, rib fractures uncommonly result from serious accidental trauma, birth related trauma, or rare genetic disorders of bone fragility.3
Rib fracture secondary to birth trauma is extremely rare. Multiple studies on birth trauma that collected data from a total of 115,756 traumatic live births showed no resulting rib fractures.4 One study that looked at rib fractures in children under 12 months of age over a 3-year period at two hospitals found that of 39 infants with rib fractures, only 2.6% of the cases were caused by birth trauma.5
The true prevalence of rib fractures secondary to birth trauma is unknown but co-occurring injuries like dystocia and clavicular fractures may support the diagnosis. A literature review performed in 2008 found 13 cases of definitive birth-related posterior rib fractures.4 In 12 of the 13 cases, the birth weight was high. In 7 cases, the birth was complicated by shoulder dystocia, as we believe occurred in the case of the first infant. And in 6 cases there a clavicle fracture was found ipsilateral to the rib fractures. Posterior rib fractures are believed to be quite specific for abuse; however, it should be noted that rib fractures that occur secondary to birth trauma are often located posteriorly as well, near the costovertebral junction.5
there is a higher prevalence of asymmetrical mid-posterior over posteromedial fractures in macrosomic neonates who are subjected to rotational forces during vaginal delivery. Ipsilateral clavicle fractures can also occur by the same mechanism. Conversely, in non-accidental trauma cases there is often a selective anterior displacement of the vertebra.4
Rib fractures may be more easily attributed to birth injury if diagnosed by radiograph while the newborn is still hospitalized after birth. Review of hospital medical records for type of delivery, infant size at birth, and a record or difficult or complicated delivery may also provide valuable information when assessing possibility of birth trauma. Newborns are handled frequently in the hours and days after birth, and an injury sustained at delivery should be quickly recognized by medical staff and parents.
Assessment for radiographic changes in fractures may also be useful when considering the possibility of birth-related trauma, as fractures will start to show periosteal reaction by approximately one week of age and will show callus formation between two and three weeks of age. Acute fractures in infants outside of the newborn period cannot reasonably be attributed to birth related trauma.
These cases highlight an important distinction between rib fractures due to birth trauma and rib fractures due to non-accidental trauma. The timing of presentation and review of birth records and radiographs can assist the clinician distinguishing abusive from non-abusive trauma.
References
- Barsness KA, Cha ES, Bensard DD, et al. The positive predictive value of rib fractures as an indicator of nonaccidental trauma in children. J Trauma. 2003 Jun;54(6):1107-10.
- Section on Radiology; American Academy of Pediatrics. Diagnostic imaging of child abuse. Pediatrics. 2009; 123(5):1430-5.
- Feldman K, Brewer, D. Child abuse, cardiopulmonary resuscitation, and rib fractures. Pediatrics 1984; 73(3):339-342.
- van Rijn RR., Bilo RAC, Robben SGF. Birth-related mid-posterior rib fractures in neonates: a report of three cases (and a possible fourth case) and a review of the literature. Pediatr Radi 2008; 39 (1): 30–34.
- Bulloch B, Shubert CJ, Brophy PD, et al. Cause and clinical characteristics of rib fractures in infants. Pediatrics 2000; 105 (4): e48.